
Abstract
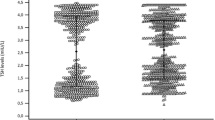
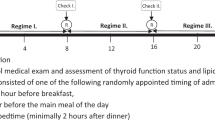
Oral levothyroxine (L-T4) is the mainstay of hypothyroidism treatment. Many factors may influence its absorption, including the timing of administration. Objective of the study is to demonstrate the therapeutic equivalence of administering liquid L-T4 with breakfast or 10 min before breakfast. This was a pilot study conducted with a crossover design AB/BA where A stays for L-T4 with breakfast and B for L-T4 10 min before breakfast. A post hoc analysis was conducted to compare L-T4 administered at breakfast or 10 min before breakfast with L-T4 administered 30 min before breakfast. Sixty-one hypothyroid patients were enrolled and assigned to one of the two treatment sequences. All patients were evaluated for TSH levels at the end of each period. Fifty-nine patients completed the study. The mean thyrotropin concentration was 1.52 ± 0.73 µU/ml when L-T4 was administered with breakfast and 1.46 ± 0.81 µU/ml when it was taken 10 min before breakfast, without clinically and statistically significant differences (P = 0.59), regardless of treatment sequence and period. The mean thyrotropin concentration was 1.54 ± 0.9 µU/ml when L-T4 was administered at 0–10 min intervals before breakfast and 1.25 ± 0.7 µU/ml when it was taken 30 min before breakfast (ratio = 1.23, within our definition of equivalence set at 0.8–1.25). There is therapeutic equivalence between liquid L-T4 administration at breakfast or 10 min before breakfast. We can also hypothesize that there are no clinically relevant differences between liquid L-T4 administration 30 min before breakfast or at shorter intervals.



Similar content being viewed by others

References
M. Centanni, A. Franchi, M.G. Santaguida, C. Virili, S. Nardo, L. Gargano, Oral thyroxine treatment: towards an individually tailored dose. Recenti Prog. Med. 98, 445–451 (2007)
R. Vita, P. Fallahi, A. Antonelli, S. Benvenga, The administration of L-thyroxine as soft gel capsule or liquid solution. Expert Opin. Drug Deliv. 11, 1103–1111 (2014)
L.H. Fish, H.L. Schwartz, J. Cavanaugh, M.W. Steffes, J.P. Bantle, J.H. Oppenheimer, Replacement dose, metabolism, and bioavailability of levothyroxine in the treatment of hypothyroidism. Role of triiodothyronine in pituitary feedback in humans. N. Engl. J. Med. 316, 764–770 (1987)
M.T. Hays, Absorption of oral thyroxine in man. J. Clin. Endocrinol. Metab. 28, 749–756 (1968)
K.W. Wenzel, H.E. Kirschsieper, Aspects of the absorption of oral L-thyroxine in normal man. Metabolism. 26, 1–8 (1977)
M.T. Hays, Localization of human thyroxine absorption. Thyroid. 1, 241–248 (1991)
M. Centanni, Thyroxine treatment: absorption, malabsorption, and novel therapeutic approaches. Endocrine 43, 8–9 (2013)
L. Liwanpo, J.M. Hershman, Conditions and drugs interfering with thyroxine absorption. Best Pract. Res. Clin. Endocrinol. Metab. 23, 781–792 (2009)
M.I. Surks, R. Sievert, Drugs and thyroid function. N. Engl. J. Med. 333, 1688–1694 (1995)
F. Santini, A. Pinchera, A. Marsili, G. Ceccarini, M.G. Castagna, R. Valeriano, M. Giannetti, D. Taddei, R. Centoni, G. Scartabelli, T. Rago, C. Mammoli, R. Elisei, P. Vitti, Lean body mass is a major determinant of levothyroxine dosage in the treatment of thyroid diseases. J. Clin. Endocrinol. Metab. 90, 124–127 (2005)
J. Jonklaas, Sex and age differences in levothyroxine dosage requirement. Endocr. Pract. 16, 71–79 (2010)
R.L. Rosenbaum, U.S. Barzel, Levothyroxine replacement dose for primary hypothyroidism decreases with age. Ann. Intern. Med. 96, 53–55 (1982)
C.T. Sawin, T. Herman, M.E. Molitch, M.H. London, S.M. Kramer, Aging and the thyroid. Decreased requirement for thyroid hormone in older hypothyroid patients. Am. J. Med. 75, 206–209 (1983)
M. Devdhar, R. Drooger, M. Pehlivanova, G. Singh, J. Jonklaas, Levothyroxine replacement doses are affected by gender and weight, but not age. Thyroid. 21, 821–827 (2011)
J.A. Loh, L. Wartofsky, J. Jonklaas, K.D. Burman, The magnitude of increased levothyroxine requirements in hypothyroid pregnant women depends upon the etiology of the hypothyroidism. Thyroid. 19, 269–275 (2009)
D.J. Lips, M.T. van Reisen, V. Voigt, W. Venekamp, Diagnosis and treatment of levothyroxine pseudomalabsorption. Neth. J. Med. 62, 114–118 (2004)
M.B. Gordon, M.S. Gordon, Variations in adequate levothyroxine replacement therapy in patients with different causes of hypothyroidism. Endocr. Pract. 5, 233–238 (2004)
L.A. Burmeister, M.O. Goumaz, C.N. Mariash, J.H. Oppenheimer, Levothyroxine dose requirements for thyrotropin suppression in the treatment of differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 75, 344–350 (1992)
M. Torlontano, C. Durante, I. Torrente, U. Crocetti, G. Augello, G. Ronga, T. Montesano, L. Travascio, A. Verrienti, R. Bruno, S. Santini, P. D’Arcangelo, B. Dallapiccola, S. Filetti, V. Trischitta, Type 2 deiodinase polymorphism (threonine 92 alanine) predicts L-thyroxine dose to achieve target thyrotropin levels in thyroidectomized patients. J. Clin. Endocrinol. Metab. 93, 910–913 (2008)
K.A. Heemstra, H.C. Hoftijzer, W.M. van der Deure, R.P. Peeters, E. Fliers, B.C. Appelhof, W.M. Wiersinga, E.P. Corssmit, T.J. Visser, J.W. Smit, Thr92Ala polymorphism in the type 2 deiodinase is not associated with T4 dose in athyroid patients or patients with Hashimoto thyroiditis. Clin. Endocrinol. 71, 279–283 (2009)
E. Lahner, C. Virili, M.G. Santaguida, B. Annibale, M. Centanni, Helicobacter pylori infection and drugs malabsorption. World J. Gastroenterol. 20, 10331–10337 (2014)
M. Centanni, L. Gargano, G. Canettieri, N. Viceconti, A. Franchi, G. Delle Fave, B. Annibale, Thyroxine in goiter, Helicobacter pylori infection, and chronic gastritis. N. Engl. J. Med. 354, 1787–1795 (2006)
S. Checchi, A. Montanaro, L. Pasqui, C. Ciuoli, V. De Palo, M.C. Chiappetta, F. Pacini, L-thyroxine requirement in patients with autoimmune hypothyroidism and parietal cell antibodies. J. Clin. Endocrinol. Metab. 93, 465–469 (2008)
C. Virili, G. Bassotti, M.G. Santaguida, R. Iuorio, S.C. Del Duca, V. Mercuri, A. Picarelli, P. Gargiulo, L. Gargano, M. Centanni, Atypical celiac disease as cause of increased need for thyroxine: a systematic study. J. Clin. Endocrinol. Metab. 97, 419–422 (2012)
M. Cellini, M.G. Santaguida, I. Gatto, C. Virili, S.C. Del Duca, N. Brusca, S. Capriello, L. Gargano, M. Centanni, Systematic appraisal of lactose intolerance as cause of increased need for oral thyroxine. J. Clin. Endocrinol. Metab. 99, 1454–1458 (2014)
T.G. Bach-Huynh, B. Nayak, J. Loh, S. Soldin, J. Jonklaas, Timing of levothyroxine administration affects serum thyrotropin concentration. J. Clin. Endocrinol. Metab. 94, 3905–3912 (2009)
R. Rajput, S. Chatterjee, M. Rajput, Can levothyroxine be taken as evening dose? Comparative evaluation of morning versus evening dose of levothyroxine in treatment of hypothyroidism. J. Thyroid Res. 505239 (2011). doi:10.4061/2011/505239
C. Cappelli, I. Pirola, E. Gandossi, A. Formenti, M. Castellano, Oral liquid levothyroxine treatment at breakfast: a mistake? Eur. J. Endocrinol. 170, 95–99 (2013)
J. Ware Jr, M. Kosinski, S.D. Keller, A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med. Care 34, 220–233 (1996)
S.S. Senn, Cross-over Trials in Clinical Research (John Wiley, Chichester, 2002)
M.P. Vanderpump, W.M. Tunbridge, J.M. French, D. Appleton, D. Bates, F. Clark, J. Grimley Evans, D.M. Hasan, H. Rodgers, F. Tunbridge, E.T. Young, The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin. Endocrinol. 43, 55–68 (1995)
C.T. Sawin, W.P. Castelli, J.M. Hershman, P. McNamara, P. Bacharach, The aging thyroid. Thyroid deficiency in the Framingham Study. Arch. Intern. Med. 145, 1386–1388 (1985)
J.G. Hollowell, N.W. Staehling, W.D. Flanders, W.H. Hannon, E.W. Gunter, C.A. Spencer, L.E. Braverman, Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J. Clin. Endocrinol. Metab. 87, 489–499 (2002)
G.J. Canaris, N.R. Manowitz, G. Mayor, E.C. Ridgway, The Colorado thyroid disease prevalence study. Arch. Intern. Med. 160, 526–534 (2000)
J.R. Garber, R.H. Cobin, H. Gharib, J.V. Hennessey, I. Klein, J.I. Mechanick, R. Pessah-Pollack, P.A. Singer, K.A. Woeber, American Association of Clinical Endocrinologists and American Thyroid Association Taskforce on Hypothyroidism in Adults, Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocr. Pract. 18, 988–1028 (2012)
M.I. Surks, E. Ortiz, G.H. Daniels, C.T. Sawin, N.F. Col, R.H. Cobin, J.A. Franklyn, J.M. Hershman, K.D. Burman, M.A. Denke, C. Gorman, R.S. Cooper, N.J. Weissman, Subclinical thyroid disease. Scientific review and guidelines for diagnosis and management. JAMA 291, 228–238 (2004)
W. Wiersinga, Thyroid hormone replacement therapy. Horm. Res. 56, 74–81 (2001)
R. Vita, G. Saraceno, F. Trimarchi, S. Benvenga, Switching levothyroxine from the tablet to the oral solution formulation corrects the impaired absorption of levothyroxine induced by proton-pump inhibitors. J. Clin. Endocrinol. Metab. 99, 4481–4486 (2014)
I. Walter-Sack, C. Clanget, R. Ding, C. Goeggelmann, V. Hinke, M. Lang, J. Pfeilschifter, Y. Tayrouz, K. Weqscheider, Assessment of levothyroxine sodium bioavailability: recommendations for an improved methodology based on the pooled analysis of eight identically designed trials with 396 drug exposures. Clin. Pharmacokinet. 43, 1037–1053 (2004)
M.G. Santaguida, C. Virili, S.C. Del Duca, M. Cellini, I. Gatto, N. Brusca, C. De Vito, L. Gargano, M. Centanni, Thyroxine softgel capsule in patients with gastric-related T4 malabsorption. Endocrine 49, 51–57 (2015)
R. Vita, G. Saraceno, F. Trimarchi, S. Benvenga, A novel formulation of L-thyroxine (L-T4) reduces the problem of L-T4 malabsorption by coffee observed with traditional tablet formulations. Endocrine 43, 154–160 (2013)
Acknowledgments
The authors would like to thank the nurse team (Nadia Biccari, Alberto Pambianco, and Lorena Urbani) of the Endocrine Clinic at the Department of Medicine, University of Perugia, for their excellent assistance. This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Morelli, S., Reboldi, G., Moretti, S. et al. Timing of breakfast does not influence therapeutic efficacy of liquid levothyroxine formulation. Endocrine 52, 571–578 (2016). https://doi.org/10.1007/s12020-015-0788-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-015-0788-2