
Abstract
Purpose
Recurrence of endometriosis after conservative surgery has been observed in 40–50 % of patients within the first 5 years. A variety of regimens such as combined oral contraceptives, GnRH agonists, danazol, and progestins have been used postoperatively to reduce recurrence rates. Oral contraceptives (oCP) have been used either in a cyclic or in a continuous (no pill-free interval) fashion. The purpose of this article was to summarize the existing evidence on the efficacy and patient compliance for the use of oCP in a continuous versus cyclic fashion following conservative surgery for endometriosis.
Methods
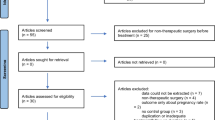
A systematic search of Medline identified four eligible studies. Studies were considered eligible, if they have evaluated oCP therapy, either in a cyclic or continuous regimen, after conservative surgery for endometriosis. Specifically, studies (1) reporting on women with endometriosis who were treated postoperatively with both continuous oCP and cyclic oCP, (2) written in English, (3) with minimum 6 months duration of medical treatment, and (4) with minimum 12 months duration of follow-up were considered eligible for our systematic review. Outcome measures of these eligible studies were tabulated and then analyzed cumulatively. A purely descriptive approach was adopted concerning all variables.
Results
Postoperative use of continuous oCP was associated with a reduction in the recurrence rate of dysmenorrhea, delay in the presentation of dysmenorrhea, reduction in nonspecific pelvic pain, and reduction in the recurrence rate for endometrioma.
Conclusions
Use of oCP in a continuous fashion following conservative surgery for endometriosis is more beneficial to cyclic use.

Similar content being viewed by others


References
Eskenazi B, Warner ML (1997) Epidemiology of endometriosis. Obstet Gynecol Clin N Am 24:235–258
Levy AR, Osenenko KM, Lozano-Ortega G, Sambrook R, Jeddi M, Belisle S et al (2011) Economic burden of surgically confirmed endometriosis in Canada. J Obstet Gynaecol Can 33:830–837
Simoens S, Dunselman G, Dirksen C, Hummelshoj L, Bokor A, Brandes I et al (2012) The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod 27:1292–1299
Sampson J (1927) Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol 14:422–469
Giudice LC (2010) Clinical practice. Endometriosis. N Engl J Med 362:2389–2398
Abbott J, Hawe J, Hunter D, Holmes M, Finn P, Garry R (2004) Laparoscopic excision of endometriosis: a randomized, placebo-controlled trial. Fertil Steril 82:878–884
Marcoux S, Maheux R, Berube S (1997) Laparoscopic surgery in infertile women with minimal or mild endometriosis. Canadian Collaborative Group on Endometriosis. N Engl J Med 337:217–222
Vercellini P, Somigliana E, Vigano P, Abbiati A, Daguati R, Crosignani PG (2008) Endometriosis: current and future medical therapies. Best Pract Res Clin Obstet Gynaecol 22:275–306
Davis L, Kennedy SS, Moore J, Prentice A (2007) Modern combined oral contraceptives for pain associated with endometriosis. Cochrane Database Syst Rev 3:CD001019
Seracchioli R, Mabrouk M, Manuzzi L, Vicenzi C, Frasca C, Elmakky A et al (2009) Post-operative use of oral contraceptive pills for prevention of anatomical relapse or symptom-recurrence after conservative surgery for endometriosis. Hum Reprod 24:2729–2735
Takamura M, Koga K, Osuga Y, Takemura Y, Hamasaki K, Hirota Y et al (2009) Post-operative oral contraceptive use reduces the risk of ovarian endometrioma recurrence after laparoscopic excision. Hum Reprod 24:3042–3048
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 62:e1–e34
Seracchioli R, Mabrouk M, Frasca C, Manuzzi L, Montanari G, Keramyda A et al (2010) Long-term cyclic and continuous oral contraceptive therapy and endometrioma recurrence: a randomized controlled trial. Fertil Steril 93:52–56
Seracchioli R, Mabrouk M, Frasca C, Manuzzi L, Savelli L, Venturoli S (2010) Long-term oral contraceptive pills and postoperative pain management after laparoscopic excision of ovarian endometrioma: a randomized controlled trial. Fertil Steril 94:464–471
Vercellini P, Frontino G, De Giorgi O, Pietropaolo G, Pasin R, Crosignani PG (2003) Continuous use of an oral contraceptive for endometriosis-associated recurrent dysmenorrhea that does not respond to a cyclic pill regimen. Fertil Steril 80:560–563
Vlahos N, Vlachos A, Triantafyllidou O, Vitoratos N, Creatsas G (2013) Continuous versus cyclic use of oral contraceptives after surgery for symptomatic endometriosis: a prospective cohort study. Fertil Steril 100:1337–1342
Clark HD, Wells GA, Huet C, McAlister FA, Salmi LR, Fergusson D et al (1999) Assessing the quality of randomized trials: reliability of the Jadad scale. Control Clin Trials 20:448–452
Chapron C, Vercellini P, Barakat H, Vieira M, Dubuisson JB (2002) Management of ovarian endometriomas. Hum Reprod Update 8:591–597
Marana R, Caruana P, Muzii L, Catalano GF, Mancuso S (1996) Operative laparoscopy for ovarian cysts. Excision vs. aspiration. J Reprod Med 41:435–438
Muzii L, Marana R, Caruana P, Catalano GF, Margutti F, Panici PB (2000) Postoperative administration of monophasic combined oral contraceptives after laparoscopic treatment of ovarian endometriomas: a prospective, randomized trial. Am J Obstet Gynecol 183:588–592
Kennedy S, Bergqvist A, Chapron C, D’Hooghe T, Dunselman G, Greb R et al (2005) ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 20:2698–2704
Jeng CJ, Chuang L, Shen J (2014) A comparison of progestogens or oral contraceptives and gonadotropin-releasing hormone agonists for the treatment of endometriosis: a systematic review. Expert Opin Pharmacother 15:767–773
Morotti M, Sozzi F, Remorgida V, Venturini PL, Ferrero S (2014) Dienogest in women with persistent endometriosis-related pelvic pain during norethisterone acetate treatment. Eur J Obstet Gynecol Reprod Biol 183:188–192
Busacca M (2006) Pain and endometriosis: an overview. J Minim Invasive Gynecol 13:573–575
Jain S, Dalton ME (1999) Chocolate cysts from ovarian follicles. Fertil Steril 72:852–856
Rodgers AK, Falcone T (2008) Treatment strategies for endometriosis. Expert Opin Pharmacother 9:243–255
Meresman GF, Auge L, Baranao RI, Lombardi E, Tesone M, Sueldo C (2002) Oral contraceptives suppress cell proliferation and enhance apoptosis of eutopic endometrial tissue from patients with endometriosis. Fertil Steril 77:1141–1147
Sesti F, Pietropolli A, Capozzolo T, Broccoli P, Pierangeli S, Bollea MR et al (2007) Hormonal suppression treatment or dietary therapy versus placebo in the control of painful symptoms after conservative surgery for endometriosis stage III–IV. A randomized comparative trial. Fertil Steril 88:1541–1547
Evans S, Moalem-Taylor G, Tracey DJ (2007) Pain and endometriosis. Pain 132(Suppl 1):S22–S25
Conflict of interest
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Zorbas, K.A., Economopoulos, K.P. & Vlahos, N.F. Continuous versus cyclic oral contraceptives for the treatment of endometriosis: a systematic review. Arch Gynecol Obstet 292, 37–43 (2015). https://doi.org/10.1007/s00404-015-3641-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-015-3641-1