
Abstract
Background and objective: Escitalopram is the most selective serotonin reuptake inhibitor antidepressant; in contrast, duloxetine inhibits both serotonin and norepinephrine reuptake. Double-blind comparison studies may help guide treatment decisions by revealing the relative benefits of different therapeutic approaches. This study evaluated the efficacy and safety of escitalopram versus duloxetine in the acute treatment of patients with moderate to severe major depressive disorder.
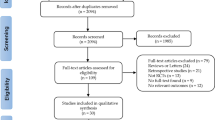
Methods: A 1-week, single-blind, placebo lead-in period followed by an 8-week, randomised, double-blind, multicentre, parallel-group comparison was conducted from 20 April 2005 to 10 March 2006 in independent psychiatric research facilities with principal investigators who were board certified in psychiatry. A total of 278 outpatients of 382 patients screened with Diagnostic and Statistical Manual of Mental Disorders (4th edition)-diagnosed major depressive disorder (Montgomery-Åsberg Depression Rating Scale [MADRS] total score ≥26) were randomised to the two treatment groups. Eight patients received no medication and were excluded from the safety group. Patients were treated with either escitalopram 10–20 mg/day (fixed at 10 mg/day for the first 4 weeks) or duloxetine 60 mg/day. The primary efficacy variable was change from baseline at week 8 in MADRS total score using the last observation carried forward (LOCF) approach. Efficacy, safety and tolerability measures were prospectively defined in the statistical analysis plan prior to study initiation unless otherwise specifically noted as conducted post hoc.
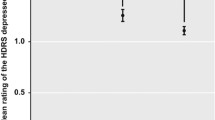
Results: A significantly greater proportion of escitalopram-treated patients completed the 8-week study compared with duloxetine-treated patients (87% vs 69%, respectively; p < 0.01). Mean baseline MADRS total scores were 31.0 for the escitalopram group and 31.6 for the duloxetine group. At week 8, escitalopram treatment resulted in significantly greater improvement compared with duloxetine on the prospectively defined primary efficacy endpoint of mean change from baseline in MADRS total score using the LOCF approach (least-squares mean difference [LSMD] −2.42; 95% CI −4.73, −0.11; p < 0.05). There was no difference between treatment groups in the observed cases (OC) analysis (LSMD −0.32; 95% CI −2.71, 2.07; p = 0.79). Significantly fewer escitalopram-treated patients discontinued because of adverse events compared with duloxetine (2% vs 13%, respectively; p < 0.01).
Conclusion: These findings suggest that escitalopram is better tolerated and at least as effective as the serotonin-norepinephrine reuptake inhibitor duloxetine in the treatment of major depressive disorder.









Similar content being viewed by others

References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. rev.: DSM-IV-R. Washington (DC): American Psychiatric Association, 2000
Murray CJL, Lopez AD, editors. The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Cambridge (MA): Harvard University Press, 1996
Wells KB, Stewart A, Hays RD, et al. The functioning and well-being of depressed patients: results from the Medical Outcomes Study. JAMA 1989 Aug; 262(7): 914–9
Kessler RC, Chiu WT, Demier O, et al. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005 Jun; 62(6): 617–27
Hirschfeld RM, Keller MB, Panico S, et al. The National Depressive and Manic-Depressive Association consensus statement on the undertreatment of depression. JAMA 1997 Jan; 277(4): 333–40
Wang PS, Lane M, Olfson M, et al. Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005 Jun; 62(6): 629–40
Delgado PL. Approaches to the enhancement of patient adherence to antidepressant medication treatment. J Clin Psychiatry 2000; 61Suppl. 2: 6–9
Keller MB, Hirschfeld RM, Demyttenaere K, et al. Optimizing outcomes in depression: focus on antidepressant compliance. Int Clin Psychopharmacol 2002 Nov; 17(6): 265–71
Masand PS. Tolerability and adherence issues in antidepressant therapy. Clin Ther 2003 Aug; 25(8): 2289–304
Bull SA, Hunkeler EM, Lee JY, et al. Discontinuing or switching selective serotonin-reuptake inhibitors. Ann Pharmacother 2002 Apr; 36(4): 578–84
Olfson M, Marcus SC, Tedeschi M, et al. Continuity of antidepressant treatment for adults with depression in the United States. Am J Psychiatry 2006 Jan; 163(1): 101–8
Geddes JR, Carney SM, Davies C, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review. Lancet 2003 Feb; 361(9358): 653–61
Kennedy S, Mclntyre R, Fallu A, et al. Pharmacotherapy to sustain the fully remitted state. J Psychiatry Neurosci 2002 Jul; 27(4): 269–80
Manning C, Marr J. ’Real-life burden of depression’ surveys: GP and patient perspectives on treatment and management of recurrent depression. Curr Med Res Opin 2003; 19(6): 526–31
Ferguson JM. SSRI antidepressant medications: adverse effects and tolerability. Prim Care Companion J Clin Psychiatry 2001 Feb; 3(1): 22–7
Hansen RA, Gartlehner G, Lohr KN, et al. Efficacy and safety of second-generation antidepressants in the treatment of major depressive disorder. Ann Intern Med 2005 Sep; 143(6): 415–26
Gardner DM, MacKinnon N, Langille DB, et al. A comparison of factors used by physicians and patients in the selection of antidepressant agents. Psychiatr Serv 2007 Jan; 58(1): 34–40
Zimmerman M, Posternak M, Friedman M, et al. Which factors influence psychiatrists’ selection of antidepressants? Am J Psychiatry 2004 Jul; 161(7): 1285–9
Owens MJ, Knight DL, Nemeroff CB. Second-generation SS-RIs: human monoamine transporter binding profile of escitalopram and R-fluoxetine. Biol Psychiatry 2001 Sep; 50(5): 345–50
Burke WJ, Gergel I, Bose A. Fixed-dose trial of the single isomer SSRI escitalopram in depressed outpatients. J Clin Psychiatry 2002 Apr; 63(4): 331–6
Wade A, Michael Lemming O, Bang Hedegaard K. Escitalopram 10 mg/day is effective and well tolerated in a placebo-controlled study in depression in primary care. Int Clin Psychopharmacol 2002 May; 17(3): 95–102
Lepola UM, Loft H, Reines EH. Escitalopram (10–20 mg/day) is effective and well tolerated in a placebo-controlled study in depression in primary care. Int Clin Psychopharmacol 2003 Jul; 18(4): 211–7
Mallinckrodt CH, Goldstein DJ, Detke MJ, et al. Duloxetine: a new treatment for the emotional and physical symptoms of depression. Prim Care Companion J Clin Psychiatry 2003 Feb; 5(1): 19–28
Mallinckrodt CH, Prakash A, Andorn AC, et al. Duloxetine for the treatment of major depressive disorder: a closer look at efficacy and safety data across the approved dose range. J Psychiatr Res 2006 Jun; 40(4): 337–48
Pritchett YL, Marciniak MD, Corey-Lisle PK, et al. Use of effect size to determine optimal dose of duloxetine in major depressive disorder. J Psychiatr Res 2007 Apr–Jun; 41(3–4): 311–8
Bielski RJ, Ventura D, Chang CC. A double-blind comparison of escitalopram and venlafaxine extended release in the treatment of major depressive disorder. J Clin Psychiatry 2004 Sep; 65(9): 1190–6
Montgomery SA, Huusom AK, Bothmer J. A randomised study comparing escitalopram with venlafaxine XR in primary care patients with major depressive disorder. Neuropsychobiology 2004; 50(1): 57–64
Nierenberg AA, Greist JH, Mallinckrodt CH, et al. Duloxetine versus escitalopram and placebo in the treatment of patients with major depressive disorder: onset of antidepressant action, a non-inferiority study. Curr Med Res Opin 2007 Feb; 23(2): 401–16
Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry 1979 Apr; 134: 382–9
Guy W. The clinician global severity and impression scales. In: ECDEU assessment manual for psychopharmacology. Washington (DC): Superintendent of Documents, US Government Printing Office, US Department of Health, Education, and Welfare Publication No. 76-338, 1976: 218–22
Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23: 56–62
Kellner R. A symptom questionnaire. J Clin Psychiatry 1987 Jul; 48(7): 268–74
Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol 1959; 32(1): 50–5
Endicott J, Nee J, Harrison W, et al. Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol Bull 1993; 29(2): 321–6
Shelton RC. The dual-action hypothesis: does pharmacology matter? J Clin Psychiatry 2004; 65Suppl. 17: 5–10
Sussman N. SNRIs versus SSRIs: mechanism of action in treating depression and painful physical symptoms. Prim Care Companion J Clin Psychiatry 2003; 5Suppl. 7: 19–26
Stahl SM, Entsuah R, Rudolph RL. Comparative efficacy between venlafaxine and SSRIs: a pooled analysis of patients with depression. Biol Psychiatry 2002 Dec 15; 52(12): 1166–74
Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001 Mar; 178: 234–41
Thase ME, Entsuah AR, Ahmed S, et al. Meta-analysis of randomized controlled trials comparing venlafaxine and SSRIs: the evidence revisited (abstract NR831). 158th Annual Meeting of the American Psychiatric Association; 2005 May 21–26; Atlanta (GA)
Detke MJ, Lu Y, Goldstein DJ, et al. Duloxetine, 60mg once daily, for major depressive disorder: a randomized double-blind placebo-controlled trial. J Clin Psychiatry 2002 Apr; 63(4): 308–15
Detke MJ, Lu Y, Goldstein DJ, et al. Duloxetine 60mg once daily dosing versus placebo in the acute treatment of major depression. J Psychiatr Res 2002 Nov–Dec; 36(6): 383–90
Lilly clinical trial registry [online]. Available from URL: http://www.lillytrials.com/results/by_product/results_cymbalta.html [Accessed 2007 Mar 7]
Menza M, Marin H, Opper RS. Residual symptoms in depression: can treatment be symptom-specific? J Clin Psychiatry 2003 May; 64(5): 516–23
Bech P, Kajdasz DK, Porsdal V. Dose-response relationship of duloxetine in placebo-controlled clinical trials in patients with major depressive disorder. Psychopharmacology (Berl) 2006 Oct; 188(3): 273–80
Dunner DL, Wohlreich MM, Mallinckrodt CH, et al. Clinical consequences of initial duloxetine dosing strategies: comparison of 30 and 60mg QD starting doses. Curr Ther Res —Clin Exp 2005; 66(6): 522–40
Psychiatric diagnosis and clinical trial completion rates: analysis of the FDA SB A reports. Neuropsychopharmacology. Epub 2007 Feb 21
Acknowledgements
This work was supported by National Institutes of Health Center Grant P30 MH 68638 and Forest Research Institute, Jersey City, NJ, USA. Dr Khan has been a principal investigator of over 200 trials sponsored by more than 40 pharmaceutical companies and has done no consulting or speaking on their behalf. He has no conflicts of interest that are directly relevant to the content of this study. Dr Alexopolous has received research grants from Cephalon and Forest Laboratories and is on speakers bureaux for Cephalon, Forest, Bristol-Myers Squibb, GlaxoSmithKline, Pfizer and Janssen. He is also a member of Forest’s scientific advisory board. Drs Bose, Li and Gandhi and Mr Gommoll are employed by Forest Research Institute.
The authors gratefully acknowledge the following study investigators for their assistance in conducting this research: Valerie Arnold, MD; Gregory Asnis, MD; Roberta R. Ball, DO; James M. Ferguson, MD; Fares J. Arguello, MD; Jerry C. Steiert, MD; Arthur J. Mollen, DO; Angela L. Pinheiro, MD; Ram K. Shrivastava, MD; Ward Smith, MD; Steven Wengel, MD and Dan Zimbroff, MD. The authors also wish to acknowledge Mary Susan Prescott, MS and Adam Ruth, PhD for their assistance in the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khan, A., Bose, A., Alexopoulos, G.S. et al. Double-Blind Comparison of Escitalopram and Duloxetine in the Acute Treatment of Major Depressive Disorder. Clin. Drug Investig. 27, 481–492 (2007). https://doi.org/10.2165/00044011-200727070-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00044011-200727070-00005