
Abstract
Objective
To assess, by smoothness index (SI), distribution of the antihypertensive effect of extended-release (ER) felodipine over 24 hours in elderly patients with hypertension.
Methods
After a 4-week washout phase, 35 elderly patients (mean age 69 ± 4 years) with mild-to-moderate hypertension received 2 weeks’ treatment with ER felodipine 5mg once daily. The dosage of ER felodipine was doubled to 10 mg/day and given for a further 2 weeks in non-responders (sitting clinic blood pressure > 140/90mm Hg). The study had an open-label design with no placebo control. After each period, clinic and ambulatory blood pressures were measured. Trough-to-peak (T/P) ratio was computed by dividing the blood pressure (BP) change at trough (22 to 24 hours after drug intake) by the change at peak (2 adjacent hours with a maximal BP reduction between the second and eighth hour after drug intake). SI was calculated as the ratio between the average of the 24, hourly, treatment-induced BP changes and its standard deviation.
Results
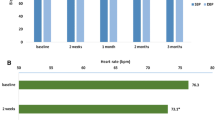
After the initial 2-week treatment period, clinic and 24-hour ambulatory BP values were higher in non-responders (145 ± 11/87 ± 8 and 135 ± 17/80 ± 6mm Hg, respectively) than in responders (133 ± 6/81 ± 3 and 130 ± 9/77 ± 7mm Hg). In non-responders, clinic and 24-hour BP values were lowered after a further 2 weeks of treatment with ER felodipine 10 mg/day (128 ± 11/78 ± 6 and 128 ± 12/75 ± 5mm Hg). SI was high in responders (0.8 ± 0.8/0.7 ± 0.7 for systolic/diastolic BP) and low in non-responders (0.5 ± 0.6/0.3 ± 0.6) during the first 2-week treatment period. It increased in non-responders after an additional 2 weeks of treatment with ER felodipine 10 mg/day (1.0 ± 0.8/0.7 ± 0.6). Median T/P ratios were 0.73 and 0.61 (systolic BP and diastolic BP) in responders and 0.41 and 0.61 in non-responders after 2 weeks of treatment. At variance with SI, T/P ratios did not increase in non-responders after doubling the dosage of ER felodipine (0.34 and 0.18). ER felodipine did not increase 24-hour heart rate. A total of nine adverse events were recorded in six patients (17%), but no patients withdrew from the study.
Conclusion
ER felodipine 5 to 10 mg/day smoothly and safely reduces 24-hour ambulatory BP in elderly patients with hypertension.






Similar content being viewed by others

References
Guidelines Subcommittee of the World Health Organization-International Society of Hypertension (WHO-ISH) Mild Hypertension Liaison Committee. 1999 World Health Organization-International Society of Hypertension Guidelines for the Management of Hypertension. J Hypertens 1999; 17: 151–83
Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure and the National High Blood Pressure Education Program Coordinating Committee. The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med 1997; 157: 2413–46
Kannel WB, Gordon T. Evaluation of cardiovascular risk in the elderly: the Framingham Study. Bull N Y Acad Med 1978; 54: 573–91
Vokonas PS, Kannel WB, Cupples LA. Epidemiology and risk of hypertension in the elderly: the Framingham Study. J Hypertens 1988; 6Suppl. 1: S3–9
Mancia G, Di Rienzo M, Grassi G, et al. Blood pressure variability and reflex control in the elderly. Aging (Milano) 1995; 7: 3–9
Lakatta EG, Cohen JD, Fleg JL, et al. Hypertension in the elderly: age- and disease-related complications and therapeutic implications. Cardiovasc Drugs Ther 1993; 7: 643–53
Casiglia E, Palatini P. Cardiovascular risk factors in the elderly. J Hum Hypertens 1998; 12: 575–81
Zanchetti A. Current position of calcium antagonists in hypertension. J Hypertens 1996; 14Suppl. 3: S11–5
Luscher TF, Cosentino F. The classification of calcium-antagonists and their selection in the treatment of hypertension: a reappraisal. Drugs 1998; 55: 509–17
Staessen JA, Fagard R, Thijs L, et al., for the Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Randomized double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350: 757–64
Hansson L, Zanchetti A, Carruthers SG, et al., for the HOT Study Group. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet 1998; 351: 1755–62
Brown MJ, Palmer CR, Castaigne A, et al. Morbidity and mortality in patients randomised to double blind treatment with a long-acting calcium-channel blocker or diuretic in the International Nifedipine GITS study: intervention as a goal in hypertension treatment (INSIGHT). Lancet 2000; 356: 366–72
Faulds D, Sorkin EM. Felodipine: a review of the pharmacology and therapeutic use of the extended release formulation in older patients. Drugs Aging 1992; 2: 374–88
van Ree JW, van der Pol GA. Low dosages of felodipine ER once daily as monotherapy in elderly hypertensive patients: effect on ambulatory blood pressure and quality of life. J Hum Hypertens 1996; 10: 613–8
Parati G, Bosi S, Castellano M, et al. Guidelines for 24h noninvasive ambulatory blood pressure monitoring: report from a working group of the Italian Society of Hypertension. High Blood Press 1995; 4: 168–74
Omboni S, Parati G, Zanchetti A, et al. Calculation of trough:peak ratio of antihypertensive treatment from ambulatory blood pressure: methodological aspects. J Hypertens 1995; 13: 1105–12
Parati G, Omboni S, Rizzoni D, et al. The smoothness index: a new, reproducible and clinically relevant measure of the homogeneity of the blood pressure reduction with treatment for hypertension. J Hypertens 1998; 16: 1685–91
Omboni S, Parati G, Mancia G. The trough:peak ratio and the smoothness index in the evaluation of control of 24h blood pressure by treatment in hypertension. Blood Press Monit 1998; 3: 201–4
Mancia G, Omboni S, Ravogli A, et al. Ambulatory blood pressure monitoring in the evaluation of antihypertensive treatment: additional information from a large data base. Blood Press 1995; 4: 148–56
Mancia G, Zanchetti A, Agabiti-Rosei E, et al., for the SAMPLE Study Group. Ambulatory blood pressure is superior to clinic blood pressure in predicting treatment-induced regression of left ventricular hypertrophy. Circulation 1997; 95: 1464–70
Fagan TC. Blood pressure reduction and tolerability of felodipine ER in older and younger hypertensive patients. The Felodipine ER in the Elderly versus Young Working Group. J Am Geriatr Soc 1997; 45: 712–7
Fagan TC, Haggert BE, Liss C. Efficacy and tolerability of extended-release felodipine and extended-release nifedipine in patients with mild-to-moderate essential hypertension. Clin Ther 1994; 16: 634–46
Hosie J, Mulder AW, Westberg B. Felodipine once daily in elderly hypertensives. Binational MC Study Group (United Kingdom and Netherlands). J Hum Hypertens 1991; 5: 49–53
Hoglund C, Hutchinson HG. A comparison of nisoldipine coat-core and felodipine in the treatment of mild-to-moderate hypertension. Int J Clin Pract 1998; 52: 221–5
Materson BJ, Reda DJ, Cushman WC, et al. Single-drug therapy for hypertension in men: a comparison of six antihypertensive agents with placebo. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. N Engl J Med 1993; 328: 914–21
Omboni S, Zanchetti A, on behalf of the Multicenter Study Investigators. Antihypertensive efficacy of lercanidipine at 2.5, 5 and 10 mg in mild to moderate essential hypertensives assessed by clinic and ambulatory blood pressure measurements. J Hypertens 1998; 16: 1831–8
Zannad F, Bernaud CM, Fay R, for the General Physician Investigators’ Group. Double-blind, randomized, multicentre comparison of the effects of amlodipine and Perindopril on 24h therapeutic coverage and beyond in patients with mild to moderate hypertension. J Hypertens 1999; 17: 137–46
Zanchetti A. The physiologic relevance of smooth twenty-four-hour blood pressure control. J Hypertens 1994; 12Suppl. 2: S17–23
Mancia G, Di Rienzo M, Parati G. Ambulatory blood pressure monitoring in hypertension research and clinical practice. Hypertension 1993; 21: 510–24
Palatini P, Penzo M, Racioppa A, et al. Clinical relevance of night-time blood pressure and day-time blood pressure variability. Arch Intern Med 1992; 152: 1855–60
Parati G, Pomidossi G, Albini F, et al. Relationship of 24h blood pressure mean and variability to severity of target organ damage. J Hypertens 1987; 5: 93–8
Frattola A, Parati G, Cuspidi C, et al. Prognostic value of 24h blood pressure variability. J Hypertens 1993; 11: 1133–7
Grossman H, Messerli FH. Effect of calcium antagonists on plasma norepinephrine levels, heart rate and blood pressure. Am J Cardiol 1997; 80: 1453–8
Kannel WB, Kannel C, Paffenbarger Jr RS, et al. Heart rate and cardiovascular mortality: the Framingham Study. Am Heart J 1987; 6: 1489–94
Palatini P, Julius S. Heart rate and the cardiovascular risk. J Hypertens 1997; 15: 3–17
Madhavan S, Ooi WL, Cohen H, et al. Relation of pulse pressure and blood pressure reduction to the incidence of myocardial infarction. Hypertension 1994; 23: 395–401
Benetos A, Rudnichi A, Safar M, et al. Pulse pressure and cardiovascular mortality in normotensive and hypertensive subjects. Hypertension 1998; 32: 560–4
Franklin SS, Khan SA, Wong ND, et al. Is pulse pressure useful in predicting coronary artery disease? The Framingham Heart Study. Circulation 1999; 100: 354–60
Zanchetti A, Bond GM, Hennig M, et al. Risk factors associated with alterations in carotid intima-media thickness in hypertension: baseline data from the European Lacidipine Study on Atherosclerosis. J Hypertens 1998; 16: 949–61
Khattar RS, Acharya DU, Kinsey C, et al. Longitudinal association of ambulatory pulse pressure with left ventricular mass and vascular hypertrophy in essential hypertension. J Hypertens 1997; 15: 737–43
Verdecchia P, Schillaci G, Borgioni C, et al. Ambulatory pulse pressure: a potent predictor of total cardiovascular risk in hypertension. Hypertension 1998; 32: 983–8
Mancia G, Omboni S, Parati G, et al. Lack of placebo effect on ambulatory blood pressure. Am J Hypertens 1995; 8: 311–5
Conway J, Coats AJS. Ambulatory blood pressure monitoring in the design of antihypertensive drug trials. J Hypertens 1991; 9Suppl.8: S57–8
Acknowledgements
No sources of funding were used to assist in the preparation of this manuscript. The authors have no conflicts of interest that are directly relevant to the content of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Antonicelli, R., Omboni, S., Di Giovanni, C. et al. Smooth Blood Pressure Control Obtained with Extended-Release Felodipine in Elderly Patients with Hypertension. Drugs Aging 19, 541–551 (2002). https://doi.org/10.2165/00002512-200219070-00007
Published:
Issue Date:
DOI: https://doi.org/10.2165/00002512-200219070-00007