
Abstract
Background
Physicians routinely factor comorbidities into diagnostic and treatment decisions. Analyses of treatment patterns and outcomes using the National Cancer Data Base (NCDB) usually adjust for comorbidities; however, the completeness of comorbidity ascertainment in the NCDB has never been assessed. We compared the prevalence of comorbidities captured in the NCDB and Surveillance, Epidemiology, and End Results (SEER)–Medicare among female breast, non-small-cell lung, and colorectal cancer patients aged ≥66.
Methods
In the NCDB, ten fields were searched for comorbidities. In the SEER–Medicare dataset, Medicare claims were used to identify comorbidities for two time periods: 12 months prior to diagnosis (Prior) and Index claim alone. Chi-square tests were used to compare comorbidity prevalence using propensity score-matched subsamples from each dataset. Kaplan–Meier survival analyses by Charlson–Deyo comorbidity score and data source were conducted.
Results
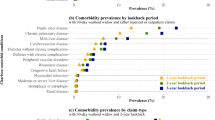
Comorbidity prevalence in NCDB did not differ significantly from that identified in SEER–Medicare Index claims across all three cancer sites, except for congestive heart failure, chronic pulmonary disease, and renal disease. However, when compared to the prevalence identified through SEER–Medicare Prior claims, comorbidity prevalence in the NCDB was lower. Overall survival rates by NCDB comorbidity scores were nearly identical to those based on SEER–Medicare Index claims but were lower than those based on SEER–Medicare Prior claims, particularly in higher comorbidity score categories.
Conclusions
The study found overall similarity of comorbidity prevalence between NCDB and SEER–Medicare Index claims, but much less similarity between NCDB and SEER–Medicare Prior claims. Future researchers should understand the limitation of comorbidities ascertained in the NCDB and interpret results accordingly.

Similar content being viewed by others


References
Lerro CC, Robbins AS, Phillips JL, Stewart AK. Comparison of cases captured in the National Cancer Data Base with those in population-based central cancer registries. Ann Surg Oncol. 2013;20(6):1759–65.
Bilimoria K, Stewart A, Winchester D, Ko C. The National Cancer Data Base: a powerful initiative to improve cancer care in the United States. Ann Surg Oncol. 2008;15(3):683–90.
Robbins AS, Pavluck AL, Fedewa SA, Chen AY, Ward EM. Insurance status, comorbidity level, and survival among colorectal cancer patients age 18 to 64 years in the National Cancer Data Base from 2003 to 2005. J Clin Oncol. 2009;27(22):3627–33.
Esnaola NF, Stewart AK, Feig BW, Skibber JM, Rodriguez-Bigas MA. Age-, race-, and ethnicity-related differences in the treatment of nonmetastatic rectal cancer: a patterns of care study from the national cancer data base. Ann Surg Oncol. 2008;15(11):3036–47.
Piccirillo JF, Costas I, Claybour P, Borah AJ, Grove L, Jeffe D. The measurement of comorbidity by cancer registries. J Registry Manage. 2003;30(1):8–14.
Gourin CG, McAfee WJ, Neyman KM, Howington JW, Podolsky RH, Terris DJ. Effect of comorbidity on quality of life and treatment selection in patients with squamous cell carcinoma of the head and neck. Laryngoscope. 2005;115(8):1371–5.
Zhu J, Fedewa S, Chen AY. The impact of comorbidity on treatment (chemoradiation and laryngectomy) of advanced, nondistant metastatic laryngeal cancer: a review of 16,849 cases from the national cancer database (2003–2008). Arch Otolaryngol Head Neck Surg. 2012;138(12):1120–8.
National Cancer Institute. SEER-Medicare linked database. Available at: http://healthservices.cancer.gov/seermedicare/. Accessed 20 Apr 2013.
Klabunde CN, Legler JM, Warren JL, Baldwin LM, Schrag D. A refined comorbidity measurement algorithm for claims-based studies of breast, prostate, colorectal, and lung cancer patients. Ann Epidemiol. 2007;17(8):584–90.
Klabunde CN, Potosky AL, Legler JM, Warren JL. Development of a comorbidity index using physician claims data. J Clin Epidemiol. 2000;53(12):1258–67.
Yan Y, Birman-Deych E, Radford MJ, Nilasena DS, Gage BF. Comorbidity indices to predict mortality from medicare data: results from the National Registry of Atrial Fibrillation. Med Care. 2005;43(11):1073–7.
Malenka D, McLerran D, Roos N, Fisher E, Wennberg J. Using administrative data to describe casemix: a comparison with the medical record. J Clin Epidemiol. 1994;47(9):1027–32.
Parsons L. Reducing bias in a propensity score matched-pair sample using greedy matching techniques. Paper presented at the 26th Annual SAS Users Group International Conference: 22–25 Apr 2001; West Sacramento, CA.
Charlson M, Pompei P, Ales K, Mackenzie C. A new method for classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–9.
National Cancer Institute. SEER-Medicare: calculation of comorbidity weights. Available at: http://healthcaredelivery.cancer.gov/seermedicare/program/comorbidity.html. Accessed 15 Jun 2011.
Bland JM, Altman DG. Multiple significance tests: the Bonferroni method. BMJ. 1995;310(6973):170.
Sanabria A, Carvalho AL, Vartanian JG, Magrin J, Ikeda MK, Kowalski LP. Comorbidity is a prognostic factor in elderly patients with head and neck cancer. Ann Surg Oncol. 2007;14(4):1449–57.
Sperling C, Noer MC, Christensen IJ, Nielsen MLS, Lidegaard Ø, Høgdall C. Comorbidity is an independent prognostic factor for the survival of ovarian cancer: a Danish register-based cohort study from a clinical database. Gynecol Oncol.2013;129(1):97–102.
Skillington S, Kallogjeri D, Lewis JS Jr, Piccirillo JF. Prognostic importance of comorbidity and the association between comorbidity and p16 in oropharyngeal squamous cell carcinoma. JAMA Otolaryngol Head Neck Surg. 2016;142(6):568–75.
Sarfati D, Koczwara B, Jackson C. The impact of comorbidity on cancer and its treatment. CA Cancer J Clin. 2016;66(4):337–50.
Sandler BJ, Wang Z, Hancock JG, Boffa DJ, Detterbeck FC, Kim AW. Gender, age, and comorbidity status predict improved survival with adjuvant chemotherapy following lobectomy for non-small cell lung cancers larger than 4 cm. Ann Surg Oncol. 2016;23(2):638–45.
Edwards BK, Noone A-M, Mariotto AB, et al. Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer. 2014;120(9):1290–314.
Patnaik JL, Byers T, DiGuiseppi C, Denberg TD, Dabelea D. The influence of comorbidities on overall survival among older women diagnosed with breast cancer. J Natl Cancer Inst. 2011;103(14): 1101–11.
Piccirillo J, Tierney R, Costas I, Grove L, Spitznagel E. Prognostic importance of comorbidity in a hospital-based cancer registry. JAMA. 2004;291(20):2441–7.
Acknowledgment
This study used the limited dataset of the NCDB and linked SEER–Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the Applied Research Program, NCI; the Office of Research, Development and Information, CMS; Information Management Services (IMS), Inc; and the SEER Program tumor registries in the creation of the SEER–Medicare database. The authors also acknowledge the efforts of the ACoS, the CoC, and the ACS in the creation of the NCDB. The ACoS and the CoC have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the authors.
Funding
This work was supported by the ACS Intramural Research Department. The funding organization had no influence on the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of interest
Chun Chieh Lin, Katherine S. Virgo, Anthony S. Robbins, Ahmedin Jemal, and Elizabeth M. Ward have no potential conflicts of interest to disclose, with the exception of those related to current or past employment. Throughout the entire project, Drs. Lin, Jemal, and Ward were ACS Intramural Research Department employees. Drs. Virgo and Robbins are previous ACS employees and no longer receive ACS support. The ACS Intramural Research Department concurrently provided ongoing financial support for the NCDB.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lin, C.C., Virgo, K.S., Robbins, A.S. et al. Comparison of Comorbid Medical Conditions in the National Cancer Database and the SEER–Medicare Database. Ann Surg Oncol 23, 4139–4148 (2016). https://doi.org/10.1245/s10434-016-5508-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5508-5