
Abstract
Background and aims
Little information exists on the relation between respiratory muscle strength such as maximum inspiratory muscle pressure (MIP) and sarcopenia in elderly cardiac patients. The present study aimed to determine the differences in MIP, and cutoff values for MIP according to sarcopenia in elderly cardiac patients.
Methods
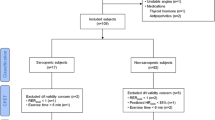
We enrolled 63 consecutive elderly male patients aged ≥65 years with cardiac disease in this cross-sectional study. Sarcopenia was defined based on the European Working Group on Sarcopenia in Older People algorithm, and, accordingly, the patients were divided into two groups: the sarcopenia group (n = 24) and non-sarcopenia group (n = 39). The prevalence of sarcopenia in cardiac patients and MIP in the patients with and without sarcopenia were assessed to determine cutoff values of MIP.
Results
After adjustment for body mass index, the MIP in the sarcopenia group was significantly lower than that in the non-sarcopenia group (54.7 ± 36.8 cmH2O; 95 % CI 42.5–72.6 vs. 80.7 ± 34.7 cmH2O; 95 % CI 69.5–92.0; F = 4.89, p = 0.029). A receiver-operating characteristic curve analysis of patients with and without sarcopenia identified a cutoff value for MIP of 55.6 cmH2O, with a sensitivity of 0.76, 1-specificity of 0.37, and AUC of 0.70 (95 % CI 0.56–0.83; p = 0.01) in the study patients.
Conclusion
Compared with elderly cardiac patients without sarcopenia, MIP in those with sarcopenia may be negatively affected. The MIP cutoff value reported here may be a useful minimum target value for identifying elderly male cardiac patients with sarcopenia.




Similar content being viewed by others


Abbreviations
- MIP:
-
Maximum inspiratory muscle pressure
- HF:
-
Heart failure
- HS:
-
Handgrip strength
- GS:
-
Gait speed
- SMI:
-
Skeletal muscle index
- BMI:
-
Body mass index
- LVEF:
-
Left ventricular ejection fraction
- FVC:
-
Forced vital capacity
- FEV1.0:
-
Forced expiratory volume in 1 s
- ANCOVA:
-
One-way analysis of covariance
- ROC:
-
Receiver-operating characteristic
- AUC:
-
Area under the curve
- SD:
-
Standard deviation
- CI:
-
Confidence interval
References
Frankenstein L, Nelles M, Meyer FJ et al (2009) Prognostic value and optimal cutoff of respiratory muscle strength in patients with chronic heart failure changes with beta-blocker treatment. Eur J Cardiovasc Prev Rehabil 16:424–429
van der Palen J, Rea TD, Manolio TA et al (2004) Respiratory muscle strength and the risk of incident cardiovascular events. Thorax 59:1063–1067
Kodric M, Trevisan R, Torregiani C et al (2013) Inspiratory muscle training for diaphragm dysfunction after cardiac surgery. J Thorac Cardiovasc Surg 145:819–823
Cruz-Jentoft AJ, Baeyens JP, Bauer JM et al (2010) European Working Group on Sarcopenia in Older People, Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing 39:412–423
Izawa KP, Watanabe S, Oka K (2015) Relationship of thresholds of physical performance to nutritional status in older hospitalized male cardiac patients. Geriatr Gerontol Int 15:189–195
Izawa KP, Watanabe S, Tochimoto S et al (2012) Relation between maximum phonation time and exercise capacity in chronic heart failure patients. Eur J Phys Rehabil Med 48:593–599
Fischer JE, Bachmann LM, Jaeschke R (2003) A readers’ guide to the interpretation of diagnostic test properties: clinical example of sepsis. Intensive Care Med 29:1043–1051
Akobeng AK (2007) Understanding diagnostic tests 3: receiver operating characteristic curves. Acta Paediatr 96:644–647
Neves LM, Karsten M, Neves VR et al (2012) Relationship between inspiratory muscle capacity and peak exercise tolerance in patients post-myocardial infarction. Heart Lung 41:137–145
Bosnak-Guclu M, Arikan H, Savci S et al (2011) Effects of inspiratory muscle training in patients with heart failure. Respir Med 105:1671–1681
Meyer FJ, Borst MM, Zugck C et al (2001) Respiratory muscle dysfunction in congestive heart failure: clinical correlation and prognostic significance. Circulation 103:2153–2158
Kim JK, Choi SR, Choi MJ et al (2014) Prevalence of and factors associated with sarcopenia in elderly patients with end-stage renal disease. Clin Nutr 33:64–68
Rolland Y, Abellan van Kan G, Gillette-Guyonnet S et al (2011) Cachexia versus sarcopenia. Curr Opin Clin Nutr Metab Care 14:15–21
Kaji H (2013) Linkage between muscle and bone: common catabolic signals resulting in osteoporosis and sarcopenia. Curr Opin Clin Nutr Metab Care 16:272–277
Lippi G, Sanchis-Gomar F, Montagnana M (2014) Biological markers in older people at risk of mobility limitations. Curr Pharm Des 20:3222–3244
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflicts of interest in relation to the work reported in this manuscript.
Funding
None.
Ethical approval
This study was approved by the St. Marianna University School of Medicine Institutional Committee on Human Research.
Statement of human and animal rights
The participants received oral explanations of the research procedures from the researchers.
Informed consent
Informed consent was obtained from each patient.
Rights and permissions
About this article

Cite this article
Izawa, K.P., Watanabe, S., Oka, K. et al. Respiratory muscle strength in relation to sarcopenia in elderly cardiac patients. Aging Clin Exp Res 28, 1143–1148 (2016). https://doi.org/10.1007/s40520-016-0534-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-016-0534-5