
Summary
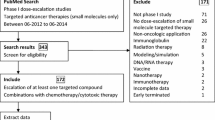
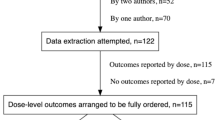
Introduction New drug development is a time- and resource-consuming process. Phase 1 trials constitute a major key-step of this development. Shortening the accrual time is of major importance. Methods 292 published phase-1-trials were retrospectively reviewed to establish the determinants of accrual time using Log-rank test and then Cox Model. Results Out of 292 trials (1997–2008), only 107 reports (36%) described the accrual time (median: 20 months, 5–72). Phase-2-recommended dose was established in 87 studies (81%). Most studies investigated regimens including cytotoxic drugs (77%) or molecular targeted therapies (29%). Under univariate analysis, two parameters shortened the accrual time: studies conducted in USA vs. other places (19 vs. 21 months p = 0.03) and regimen with more than 2 dose-escalated drugs (13 vs. 21 months, p = 0.003). One parameter was significantly associated with longer accrual time: starting dose justified by animal toxicology data vs. previous clinical trials (22 vs. 19 months, p = 0.03). Most of parameters did not significantly affect the accrual time: nature of investigated drugs, duration of treatment cycle, phase 1 dedicated to specific tumoral subtypes, number of centers, method of drug escalation (classical 3+3 vs. accelerated titration design), type of increment (modified Fibonacci method vs. others) and presence of expansion of cohort at the phase-II-recommended dose. Cox model analysis retained one determinant: starting dose justified by animal toxicology data: HR = 2.00 [1.45–5.20], p = 0.047. Conclusion Few parameters influence the accrual time of dose-escalation phase-1 trials. Real first-in-man phase 1 studies based on starting dose estimated from animal toxicological data require longer accrual time.


Similar content being viewed by others

References
Lipsett MB (1982) On the nature and ethics of phase I clinical trials of cancer chemotherapies. JAMA 248:941–942
Ratain MJ, Mick R, Schilsky RL et al (1993) Statistical and ethical issues in the design and conduct of phase I and II clinical trials of new anticancer agents. J Natl Cancer Inst 85:1637–1643
Penel N, Vanseymortier M, Bonneterre ME, Clisant S, Dansin E, Vendel Y, Beuscart R, Bonneterre J (2008) Prognostic factors among cancer patients with good performance status screened for phase I trials. Invest New Drugs 26:53–58
Arkenau HT, Olmos D, Ang JE, Judson I, Kaye B (2008) Clinical outcome and prognostic factors for patients treated within the context of a phase I study: the Royal Marsden Hospital experience. Br J Cancer 98:1029–1033
Simon R, Friedlin B, Rubinstein LV, Arbuck SG, Collins J, Christian MC (1997) Accelerated titration designs for phase I clinical trials in oncology. J Natl Cancer Inst 89:1138–1147
O’Quigley J, Pepe M, Fisher L (1990) Continual reassessment method: a practical design for phase 1 clinical trials in cancer. Biometrics 46:33–48
Collins JM, Grieshaber CK, Chabner BA (1990) Pharmacologically guided phase 1 clinical trials based on preclinical development. J Natl Cancer Inst 82:1321–1326
Verweij J (2008) “No risk, no fun”: challenges for the oncology phase I clinical trial time-performance. Eur J Cancer 44:2600–2607
Kelloff GK, Sigman CC (2005) New science-based endpoints to accelerate oncology drug development. Eur J Cancer 41:491–501
Kaplan EL, Meier P (1958) Nonparametric estimation from incomplete observations. J Am Stat Assoc. 53:457–481
Mantel N (1966) Estimation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep. 50:163–170
Cox D (1972) Regression models and life tables (with discussion). J R Stat Soc B 34:187–220
Kerr DJ (1995) Phase I clinical trials: adapting methodology to face new challenges. Ann Oncol 5:S67–S70
Dent SF, Einsenhauer EA (1996) Phase I trial design: are new methodologies begin put into practice? Ann Oncol 7:561–566
Horstmann E, McCabe MS, Grochow L et al (2005) Risks and benefits of phase 1 oncology trials, 1991 through 2002. N Engl J Med 352:895–904
Penta JS, Rozencweig M, Guarino AM et al (1979) Mouse and large-animal toxicology studies of twelve antitumor agents: relevance of starting dose for phase I clinical trials. Cancer Chemother Pharmacol 31:247–250
Penta JS, Rosner GL, Trump DL (1992) Choice of the starting dose and escalation for phase I clinical studies of antitumour agents. Cancer Chemother Pharmacol 31:247–250
Dowlati A, Manda S, Gibbons J et al (2008) Multi-institutional phase I trials of anticancer agents. J Clin Oncol 26:1926–1931
Penel N, Isambert N, Leblond P et al (2009) “classical 3+3 design” versus “accelerated titration designs”: analysis of 270 phases I trials investigating anti-cancer agents. Invest New Drugs, doi:10.1007/s10637-008-9213-5
Penel N, Adenis A (2009) Publication biases and phase II trials investigating anticancer therapies. Invest New Drugs 27:287–288
Bonneterre J, Adenis A, Dansin E et al (2009) Is the maximal tolerated dose still the best primary endpoint ? Analysis of 288 dose-seeking phase I trials (abstract 2513). J Clin Oncol 27(supplS7) abstr 2513
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Penel, N., Leblond, P., Lansiaux, A. et al. Justification of the starting dose as the main determinant of accrual time in dose-seeking oncology phase 1 trials. Invest New Drugs 28, 839–843 (2010). https://doi.org/10.1007/s10637-009-9317-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-009-9317-6