
Abstract
Purpose
To evaluate the diagnosis, epidemiology, risk factors, and treatment of chylous ascites after colorectal cancer surgery.
Methods
Among 907 patients who underwent colorectal cancer resection at our institution between 2006 and 2009, chylous ascites developed in 9. We analyzed the clinical data for these 9 patients.
Results
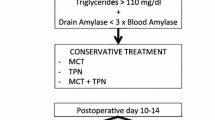
Five of the nine patients with chylous ascites had undergone right hemicolectomy and seven had undergone D3 lymph node dissection. In all patients, chylous ascites began to develop the day after commencement of oral intake or the next day. Two patients had no change in diet, one was started on a high-protein and low-fat diet, and six were put on intestinal fasting. Drainage tubes were removed within 5 days after treatment in seven patients. The hospital stay was about 2 weeks after surgery and 1 week after treatment. We found that the tumor area, tumors fed by the superior mesenteric artery, and D3 lymph node dissection were significantly associated with chylous ascites.
Conclusions
Chylous ascites after colorectal cancer surgery occurred at an incidence of 1.0%, but was significantly more frequent after surgery for tumors fed by the superior mesenteric artery and after D3 lymph node dissection. Conservative treatment was effective in all cases.

Similar content being viewed by others


References
Kaas R, Rustman LD, Zoetmulder FA. Chylous ascites after oncological abdominal surgery: incidence and treatment. Eur J Surg Oncol. 2001;27(2):187–9.
Cardenas A, Chopra S. Chylous ascites. Am J Gastroenterol. 2002;97(8):1896–900.
Noel AA, Gloviczki P, Bender CE, Whitley D, Stanson AW, Deschamps C. Treatment of symptomatic primary chylous disorders. J Vasc Surg. 2001;34(5):785–91.
Campisi C, Bellini C, Eretta C, Zilli A, da Rin E, Davini D, et al. Diagnosis and management of primary chylous ascites. J Vasc Surg. 2006;43(6):1244–8.
Aalami OO, Allen DB, Organ CH Jr. Chylous ascites: a collective review. Surgery. 2000;128(5):761–78.
Leibovitch I, Mor Y, Golomb J, Ramon J. The diagnosis and management of postoperative chylous ascites. J Urol. 2002;167(2 Pt 1):449–57.
JSCCR guidelines 2010 for the treatment of colorectal cancer. Japanese Society for Cancer of the Colon and Rectum.
Giovannini I, Giuliante F, Chiarla C, Ardito F, Vellone M, Nuzzo G. Non-surgical management of a lymphatic fistula, after laparoscopic colorectal surgery, with total parenteral nutrition, octreotide, and somatostatin. Nutrition. 2005;21(10):1065–7.
Giovannini I, Giuliante F, Chiarla C, Giordano M, Ardito F, Vellone M, et al. External lymphatic fistula after intra-abdominal lymphadenectomy for cancer. Treatment with total parenteral nutrition and somatostatin. Nutrition. 2008;24(11–12):1220–3.
Mincher L, Evans J, Jenner MW, Varney VA. The successful treatment of chylous effusions in malignant disease with octreotide. Clin Oncol (R Coll Radiol). 2005;17(2):118–21.
Nishizawa K, Ito N, Yamamoto S, Kamoto T, Ogawa O. Successful laparoscopic management of chylous ascites following laparoscopic radical nephrectomy. Int J Urol. 2006;13(5):619–21.
Chan KY, Teoh CM, Sukumar N. Chylous ascites after anterior resection for rectal carcinoma: a rare but significant incident. Asian J Surg. 2006;29(1):46–8.
Sugiyama S, Tutumi N, Yokomizo H, Nakajima E, Mishima S, et al. Clinical study of cases on chylous ascites following surgery. Surgical therapy. 2007;96(5):974–7.
Ablan CJ, Littooy FN, Freeark RJ. Postoperative chylous ascites: diagnosis and treatment. A series report and literature review. Arch Surg. 1990;125(2):270–3.
Kuroda S, Aoki H, Shiozaki S, Harano M, Sasaki H, et al. Clinical study on chylous acites following hepato-pancreatic surgery. Jpn Soc Gastroenterol Surg. 2006;39(5):631–6.
Yol S, Bostanci EB, Ozogul Y, Ulas M, Akoglu M. A rare complication of D3 dissection for gastric carcinoma: chyloperitoneum. Gastric Cancer. 2005;8(1):35–8.
Maeta M, Yamashiro H, Saito H, Katano K, Kondo A, Tsujitani S, et al. A prospective pilot study of extended (D3) and superextended para-aortic lymphadenectomy (D4) in patients with T3 or T4 gastric cancer managed by total gastrectomy. Surgery. 1999;125(3):325–31.
Shimizu K, Yoshida J, Nishimura M, Takamochi K, Nakahara R, Nagai K. Treatment strategy for chylothorax after pulmonary resection and lymph node dissection for lung cancer. J Thorac Cardiovasc Surg. 2002;124(3):499–502.
Bolger C, Walsh TN, Tanner WA, Keeling P, Hennessy TP. Chylothorax after oesophagectomy. Br J Surg. 1991;78(5):587–8.
Neyer M, Peschel R, Akkad T, Springer-Stohr B, Berger A, Bartsch G, et al. Long-term results of laparoscopic retroperitoneal lymph-node dissection for clinical stage I nonseminomatous germ-cell testicular cancer. J Endourol. 2007;21(2):180–3.
Evans JG, Spiess PE, Kamat AM, Wood CG, Hernandez M, Pettaway CA, et al. Chylous ascites after post-chemotherapy retroperitoneal lymph node dissection: review of the M.D. Anderson experience. J Urol. 2006;176(4 Pt 1):1463–7.
Kamiya K, Unno N, Konno H. Intraoperative indocyanine green fluorescence lymphography, a novel imaging technique to detect a chyle fistula after an esophagectomy: report of a case. Surg Today. 2009;39(5):421–4.
Kenney PA, Tuerk IA. Complications of laparoscopic retroperitoneal lymph node dissection in testicular cancer. World J Urol. 2008;26(6):561–9.
Conflict of interest
None of the authors have a conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nishigori, H., Ito, M., Nishizawa, Y. et al. Postoperative chylous ascites after colorectal cancer surgery. Surg Today 42, 724–728 (2012). https://doi.org/10.1007/s00595-012-0132-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-012-0132-x