
Abstract
Objectives
To evaluate differences in the tumor response classifications that result from clinical measurements and to compare these response classifications with overall survival for patients with malignant pleural mesothelioma (MPM).
Methods
One hundred thirty-one computed tomography (CT) scans were collected from 41 MPM patients enrolled in a clinical trial. Primary measurements had been acquired by clinical radiologists at a single center during routine clinical workflow, and the variability of these measurements was investigated. Retrospective measurements were acquired by a single radiologist in compliance with the study protocol based on the modified response evaluation criteria in solid tumors (RECIST). Differences in response classification categories by the two measurement approaches were evaluated and compared with patient survival.
Results
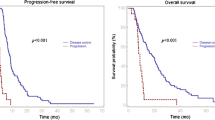
Eleven (27%) of the 41 MPM patients had primary measurements at baseline or at follow-up that deviated from the guidelines of the clinical trial protocol. Among the 41 baseline scans, no statistical difference was observed in summed tumor measurements between primary and retrospective measurements. Response classification based on primary and retrospective measurements was different in 23 (26%) of the 90 follow-up scans, and best response was the different in seven (17%) of the 41 patients. Using Harrell’s C statistic as a measure of correlation, response based on retrospective measurements correlated better with survival (C = 0.62) than did response based on primary measurements (C = 0.57).
Conclusions
Strict compliance with the measurement protocol yields tumor response classifications that may differ from those obtained in clinical practice. Response based on retrospective measurements correlated better with survival than did response based on primary measurements.
Key Points
• Response classifications could be different between clinical primary and retrospective measurements for malignant pleural mesothelioma.
• Response classifications obtained by strict compliance with the trial-specific protocol correlated better with survival than the classifications based on primary measurements.
• Quality assurance and radiologist training measures should be used to ensure the integrity of image-based tumor measurements in mesothelioma clinical trials.



Similar content being viewed by others
Abbreviations
- CT:
-
Computed tomography
- MPM:
-
Malignant pleural mesothelioma
- RECIST:
-
Response evaluation criteria in solid tumors
References
Therasse P, Arbuck AG, Eisenhauer EA et al (2000) New guidelines to evaluate the response to treatment in solid tumor. J Natl Cancer Inst 92:205–216
Eisenhauer EA, Therasse P, Bogaerts J et al (2009) New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). Eur J Cancer 45:228–247
Hopper KD, Kasales CJ, van Slyke MA, Schwartz TA, TenHave TR, Jozefiak JA (1996) Analysis of interobserver and intraobserver variability in CT tumor measurements. AJR Am J Roentgenol 167:851–854
Thiesse P, Ollivier L, Di Stefano-Louineau D et al (1997) Response rate accuracy in oncology trials: reasons for interobserver variability. J Clin Oncol 15:3507–3514
Muenzel D, Engels HP, Bruegel M, Kehl V, Rummeny EJ, Metz S (2012) Intra- and inter-observer variability in measurement of target lesions: implication on response evaluation according to RECIST 1.1. Radiol Oncol 46:8–18
Byrne MJ, Nowak AK (2004) Modified RECIST criteria for assessment of response in malignant pleural mesothelioma. Ann Oncol 15:257–260
Armato SG 3rd, Oxnard GR, MacMahon H et al (2004) Measurement of mesothelioma on thoracic CT scans: a comparison of manual and computer-assisted techniques. Med Phys 31:1105–1115
Armato SG 3rd, Ogarek JL, Starkey A et al (2006) Variability in mesothelioma tumor response classification. AJR Am J Roentgenol 186:1000–1006
Armato SG 3rd, Nowak AK, Francis RJ, Kocherginsky M, Byrne MJ (2014) Observer variability in mesothelioma tumor thickness measurements: defining minimally measurable lesions. J Thorac Oncol 9:1187–1194
Krug LM, Kindler HL, Calvert H et al (2015) Vorinosat in patients with advanced malignant pleural mesothelioma who have progressed on previous chemotherapy (VANTAGE-014): a phase 3, double-blind, randomized, placebo-controlled trial. Lancet Oncol 16:447–456
Harrell FE Jr, Lee KL, Mark DB (1996) Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med 15:361–387
Ford R, Schwartz L, Dancey J et al (2009) Lessons learned from independent central review. Eur J Cancer 45:268–274
Dodd LE, Korn EL, Freidlin B et al (2008) Blinded independent central review of progression-free survival in phase III clinical trials: important design element or unnecessary expense? J Clin Oncol 26:3791–3796
Amit O, Mannino F, Stone AM et al (2011) Blinded independent central review of progression in cancer clinical trials: results from a meta-analysis. Eur J Cancer 47:1772–1778
Jain RK, Lee JJ, Ng C et al (2012) Change in tumor size by RECIST correlates linearly with overall survival in phase I oncology studies. J Clin Oncol 30:2684–2690
Labby ZE, Armato SG 3rd, Kindler HL, Dignam JJ, Hasani A, Nowak AK (2012) Optimization of response classification criteria for patients with malignant pleural mesothelioma. J Thorac Oncol 7:1728–1734
Liu F, Zhao B, Krug LM et al (2010) Assessment of therapy response and prediction of survival in malignant pleural mesothelioma through computer-aided volumetric measurement on computed tomography scans. J Thorac Oncol 5:879–884
Ak G, Metintas M, Metintas S, Yildirim H, Ozkan R, Ozden H (2010) Three-dimensional evaluation of chemotherapy response in malignant pleural mesothelioma. Eur J Radiol 74:130–135
Gill RR, Richards WG, Yeap BY et al (2012) Epithelial malignant pleural mesothelioma after extrapleural pneumonectomy: stratification of survival with CT-derived tumor volume. AJR Am J Roentgenol 198:359–363
Labby ZE, Nowak AK, Dignam JJ, Straus C, Kindler HL, Armato SG 3rd (2013) Disease volumes as a marker for patient response in malignant pleural mesothelioma. Ann Oncol 24:999–1005
Francis RJ, Byme MJ, van der Schaaf AA et al (2007) Early prediction of response to chemotherapy and survival in malignant pleural mesothelioma using a novel semiautomated 3-dimensional volume-based analysis of serial 18F-FDG PET scans. J Nucl Med 48:1449–1458
Cheng L, Tunariu N, Collins DJ et al (2015) Response evaluation in mesothelioma: beyond RECIST. Lung Cancer 90:433–441
Acknowledgements
This study has been presented in part at the RSNA 2011 meeting.
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Feng Li.
Conflict of interest
The authors of this manuscript declare relationships with the following companies: Dr. Armato is a consultant for Aduro Biotech, Inc. Dr. MacMahon is a shareholder of Hologic and a consultant for Riverain Technologies. Drs. Li, Armato, and MacMahon receive royalties and licensing fees for computer-aided diagnosis technology through The University of Chicago. Dr. Kindler is a consultant for Merck and receives research support from Merck.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• Retrospective
• Cross sectional study
• Performed at one institution
Rights and permissions
About this article

Cite this article
Li, F., Ahmad, M., Qayyum, F. et al. Correlation of patient survival with clinical tumor measurements in malignant pleural mesothelioma. Eur Radiol 29, 2981–2988 (2019). https://doi.org/10.1007/s00330-018-5887-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5887-z