
Abstract
Background
The technique of X-ray-based dual photon absorptiometry (DXA) is frequently used in children for the detection of changes in bone mass or body composition. Such changes can only be considered real if the uncertainties arising from the measurement technique are exceeded.
Objective
Our objectives were twofold: (1) to determine the reproducibility of bone mineral density (BMD) measurements in children at the spine and the hip and from the whole body, as well as of whole-body measurements of mineral mass, lean body mass and fat mass in children; and (2) to estimate, from the measured precision, the time interval that needs to elapse before a statistically significant change in a DXA variable can be detected.
Materials and methods
The reproducibility of techniques for the measurement of BMD and body composition using DXA was measured in 15 young children (9 girls and 6 boys) and 17 older children (9 girls and 8 boys).
Results
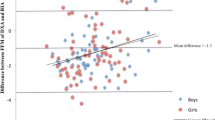
Reproducibility was derived from the standard deviation of three repeated measurements of spine BMD, total hip BMD, whole-body BMD (WBBMD), whole-body bone mineral content (WBBMC), lean mass and fat mass. Technique precision was better than 0.01 g cm−2 for spine BMD and for WBBMD. Hip BMD measurements were slightly less precise, particularly in younger children (0.013 g cm−2). For body composition variables, technique precision was 13 g for WBBMC, 201 g for lean body mass and 172 g for fat mass in younger children. Technique precision for older children was 18 g, 251 g and 189 g for the corresponding variables. Predictions showed that the absence of a normal increase in WBBMC in a small-for-age girl could be established after 12 months. For spine BMD, a significant increase should be observable after 6 months for boys over the age of 11 years. For younger boys, more than 12 months has to elapse before anticipated changes can be detected with confidence.
Conclusion
The time intervals required to elapse before decisions can be made concerning the significance of observed differences between successive measurements of BMD or body composition in children depend upon the age of the child.


Similar content being viewed by others


References
Binkovitz LA, Henwood MJ (2007) Pediatric DXA: technique and interpretation. Pediatr Radiol 37:21–31
Baim A, Wilson CR, Lewiecki EM et al (2005) Precision assessment and radiation safety for dual-energy X-ray absorptiometry. J Clin Densitom 8:371–378
Glüer CC, Blake G, Lu Y et al (1995) Accurate assessment of precision errors: how to measure the reproducibility of bone densitometry techniques. Osteoporos Int 5:262–270
Shepherd JA, Lu Y, Wilson K et al (2006) Cross-calibration and minimum precision standards for dual-energy X-ray absorptiometry: the 2005 ISCD official positions. J Clin Densitom 9:31–36
Sala A, Webber CE, Morrison J et al (2007) Whole-body bone mineral content, lean body mass, and fat mass measured by dual-energy X-ray absorptiometry in a population of normal Canadian children and adolescents. Can Assoc Radiol J 58:46–52
Webber CE, Beaumont LF, Morrison J et al (2007) Age-predicted values for lumbar spine, proximal femur, and whole-body bone mineral density: results from a population of normal children aged 3 to 18 years. Can Assoc Radiol J 58:37–45
Centers for Disease Control and Prevention (2008) 2000 CDC growth charts: clinical growth charts. National Center for Health Statistics, Hyattsville, MD. http://www.cdc.gov/growthcharts Accessed 17 November 2008
Lodder MC, Lems WF, Ader HJ et al (2004) Reproducibility of bone mineral density measurement in daily practice. Ann Rheum Dis 63:285–289
Margulies L, Horlick M, Thornton JC et al (2005) Reproducibility of pediatric whole body bone and body composition measures by dual-energy X-ray absorptiometry using the GE Lunar Prodigy. J Clin Densitom 8:298–304
Hammami M, Koo WW, Hockman EM (2004) Technical considerations for fan-beam dual-energy X-ray absorptiometry body composition measurements in pediatric studies. J Parenter Enteral Nutr 28:328–333
Webber CE (2006) Photon absorptiometry, bone densitometry and the challenge of osteoporosis. Phys Med Biol 51:R169–R185
Ravaud P, Reny JL, Giraudeau B et al (1999) Individual smallest detectable difference in bone mineral density measurements. J Bone Miner Res 14:1449–1456
Cummings SR, Black D (1986) Should perimenopausal women be screened for osteoporosis? Ann Intern Med 104:817–823
Author information
Authors and Affiliations
Corresponding author
Appendix: derivation of DXA reproducibility
Appendix: derivation of DXA reproducibility
Recommended procedures for the evaluation of reproducibility with DXA require repeated measurements on phantoms or human volunteers; reproducibility or precision is given by the standard deviation of the series of measurements. When a phantom is used as the test object, the standard deviation will not include any contribution from subject positioning. Short-term precision is the reproducibility calculated from measurements repeated immediately after repositioning a subject rather than a phantom. Inevitably, short-term precision will be worse than the precision determined from a phantom. Long-term precision is the reproducibility calculated from subject measurements repeated after intervals approaching or exceeding 1 year. The relevant parameter for clinical application of DXA techniques is the long-term precision. However, because measurement of long-term precision is challenging, common practice is to measure in vivo short-term reproducibility and to evaluate long-term stability of DXA equipment from phantom measurements.
Frequently, the standard deviation is expressed as a percentage of the mean value; that is, the CV. Values of CV for lumbar spine BMD measured in phantoms are typically 0.5%. Short-term precision in adults is normally about 1% while long-term in vivo precision is closer to 2% [11]. In children and in adults with osteoporosis, CV has the disadvantage that reproducibility may appear to be worse simply because BMD is smaller and not because the measurements are less reproducible [12]. For example, if the standard deviation of repeated measurements is 0.01 g cm−2, the short-term precision in adults would be about 1% when expressed as a CV whereas in a 3-year-old child, the same standard deviation would yield a CV of about 2.5%. Precision is also frequently expressed as the ICC, which is the proportion of the variance that can be attributed to the subjects expressed as a fraction of the total variance arising from the technique plus that from the subjects. Consequently, the closer the ICC is to unity, the smaller the technique variance.
In this study, short-term precision for each subject was expressed as the standard deviation of the three measurements for each variable. That is, subject precision is given by:
where x i is each of the three measurements for a given variable and \(\bar x\) is the mean of the three measurements. The denominator includes the number of measurements (n=3) and expresses the number of degrees of freedom for each subject. Technique precision (TP) is given by an appropriate combination of the precision determined for each subject. Since it is the subject variances that should be averaged, the technique precision is obtained from:
where N is the number of subjects. In this study, TP was determined for groups of both younger and older children. Confidence intervals for TP were evaluated from the expression:
where df is the total number of degrees of freedom (=2×N) and χ2 is the critical value corresponding to either the probability of exceeding 97.5% or the critical value for falling below 2.5% of the chi-squared distribution.
Establishment of the technique precision allows the derivation of the smallest difference between successive measurements that can be considered statistically significant at the 95% confidence level [13]. This difference is given by 1.96×(TP2 + TP2)½ and is known as the smallest detectable difference (SDD) or the least significant change (LSC). When applied to BMD, the units of the SDD and the LSC are both grams per centimeter squared.
Rights and permissions
About this article
Cite this article
Leonard, C.M., Roza, M.A., Barr, R.D. et al. Reproducibility of DXA measurements of bone mineral density and body composition in children. Pediatr Radiol 39, 148–154 (2009). https://doi.org/10.1007/s00247-008-1067-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-008-1067-7