
Abstract
Objective
The aim of the study was to evaluate the usage pattern of nonsteroidal anti-inflammatory drugs (NSAIDs) in diverse clinical practice settings in India.
Methods
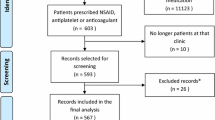
The study was conducted in Mumbai city and its suburbs, involving 1,916 doctors from among general practice to specialist practice. The data were collected with the help of a semi-structured questionnaire and were analysed statistically to bring out differences in NSAID usage among different groups of prescribers.
Results
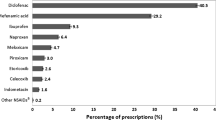
All the 1,916 doctors prescribed NSAIDs frequently with prescriptions ranging from 1 to 15 daily; they short-listed and prescribed only two to five NSAIDs from among a plethora of drugs available including fixed-dose combinations (FDCs). It is significant that FDCs were prescribed by more than 39% of doctors in all the categories, the highest prescribers being orthopaedic surgeons (76%) and lowest general practitioners (GPs; 39%). Apart from recommended usage, NSAIDs such as ibuprofen, diclofenac and aspirin were used for pelvic inflammatory disease, and indomethacin for pre-term labour and patent ductus arteriosus. Dosage variation, both in terms of dose and frequency of administration, has been observed for several NSAIDs in the GPs category as well as in the specialist categories—except that of paediatricians. In patients suffering from bronchial asthma, there has been significant use of aspirin and ibuprofen by GPs despite contra-indication for their use in such patients. Most prescribers perceived that NSAIDs are associated with mild gastrointestinal (GI) adverse events. Ibuprofen, a drug with reportedly better gastric tolerance, was perceived to cause GI adverse events, though to a lesser extent than aspirin; fewer prescribers perceived that diclofenac and piroxicam cause GI adverse events when compared with aspirin and ibuprofen. There were significant differences among the five practice categories with regard to preferences for NSAIDs. The first choice NSAIDs were ibuprofen, aspirin, diclofenac, paracetamol, piroxicam and ibuprofen+paracetamol FDC.
Conclusions
This study has shown that there exist significant differences in the usage pattern and preferences of NSAIDs among different practice categories in India. The data have also revealed that there is a need for awareness programmes on rational prescribing of NSAIDs towards optimal therapeutics and improved patient care in India.


Similar content being viewed by others
References
Laurence DR, Bennett PN, Brown MJ (1997) Inflammation, arthritis and anti-inflammatory drugs (NSAIDs). In: Clinical pharmacology, 8th edn. Churchill Livingstone, Edinburgh, pp 249–266
Roberts LJ, Morrow JD (2001) Analgesic-antipyretic and anti-inflammatory agents and drugs employed in the treatment of gout. In: Hardman JG et al. (eds) Goodman and Gilman’s. The pharmacological basis of therapeutics, 10th edn. McGraw-Hill, New York, pp 687–731
AUDIT Commission (1994) A prescription for improvement, towards more rational prescribing in general practice. Audit Commission, London, pp 15–41
Prescription Analysis and CosT (PACT) (1996) Are NSAIDs being over prescribed? Pharm J 256:331 (cited in Inpharma 1996 No.1029: 7)
de Vries TPGM, Henning RH, Hogerzeil HV, Fresle DA (1995) Selecting your P(ersonal) drugs. In WHO guide to good prescribing—a practical manual. World Health Organization, Geneva
Bhattacharya SK, Roy K (1994) Is Indian pain more painful? Bull Drug Health Inform 1(1):8
American Medical Association (1995) Antiarthritic drugs. In: Drug evaluations annual, pp 1875–1924
Beaver WT (1984) Combination analgesics. Am J Med 80:38–53
Dahanukar SA, Rege NN (1998) Focus on NSAID combinations. Ind Pract 51(1):43–47
Pearce JM (1990) Pelvic inflammatory disease. BMJ 300:1090–1091
Dodson MG (1990) Optimum therapy for acute pelvic inflammatory disease. Drugs 39(4):511–522
Anonymous (1994) Rational use of NSAIDs for musculoskeletal disorders. Drug Ther Bull 32(12):91–95
Langman MJS, Weil J, Wainwright P, Lawson DH, Rawlins MD, Logan RFA, Murphy M, Vessey MP, Colin-Jones DG (1994) Risks of bleeding peptic ulcer associated with individual nonsteroidal anti-inflammatory drugs. Lancet 343:1075–1078
Fenner R, Mann RD (1997) Drug safety and pharmacovigilance. In: Page CP et al (eds) Integrated pharmacology. Mosby, London, pp 83–90
Read JL, Epstein (1984) Aspirin and its expensive substitutes: prescribing patterns and cost implications. J Comm Health 9(3):216–221
Keys J, Bearden PHG, Lau C, Lang CC, McDevitt DG (1992) General Practitioners’ use of nonsteroidal anti-inflammatory drugs in Tayside and Fife regions. J Roy Soc Med 85:442–445
Calin A (1987) Rational Prescribing of NSAIDs. MIMS Magazine 1September:24–29
Day, RO, Graham GG, Williams KM, Brooks PM (1988) Variability in response to NSAIDs fact or fiction? Drugs 36:643–651
Brooks PM, Day RO (1991) Nonsteroidal anti-inflammatory drugs- differences and similarities. N Engl J Med 324(24):1716–1725
Acknowledgements
This study was undertaken by the first author in fulfillment of the requirements for the degree of Doctor of Philosophy (Faculty of Medicine) of the University of Mumbai. The authors wish to thank the Dean, L.T.M. Medical College & L.T.M.G. Hospital, Sion, Mumbai for the use of various facilities of the institution, Mr. A. R. Kannappan, Biometrician for help in statistical analysis of the data and all the doctors who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Paul, A.D., Chauhan, C.K. Study of usage pattern of nonsteroidal anti-inflammatory drugs (NSAIDs) among different practice categories in Indian clinical setting. Eur J Clin Pharmacol 60, 889–892 (2005). https://doi.org/10.1007/s00228-004-0849-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-004-0849-6