
Abstract
Purpose
We investigated the spontaneous recovery of non-operated traumatic brachial plexus injury (BPI).
Methods
A total of 25 cases of non-operated traumatic BPI were analysed by retrospective review of medical records; in all cases, consecutive electrodiagnostic studies (ES) were conducted from 1 to 4 months and 18 to 24 months post-trauma. Injury severity was assessed using a modified version of Dumitru and Wilbourn’s scale (DWS) based on ES. Spontaneous recovery of brachial plexus components per subject was analysed using Wilcoxon’s signed-rank test. A two-tailed Fisher’s exact or Pearson’s Chi-square test was used to examine the associations between initial injury severity (DWS grade 2 vs. 3, complete vs. incomplete), accompanying injury type (open vs. closed), main lesion location (supraclavicular vs. infraclavicular lesion), and spontaneous recovery.
Results
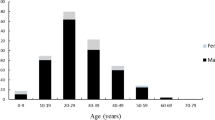
The most common cause of BPI was traffic accident (TA) (15 cases, 60%), and the most common type of TA-induced BPI was a motorcycle TA (5 cases), accounting for 20% of all injuries. The second most common type of injury was an occupational injury (6 cases, 24%). Thirty-eight (69%) of 55 injured brachial components in 25 cases had DWS grade 3 and 17 brachial components (31%) had grade 2. The DWS grade of brachial plexus components per subject significantly differed between the first and follow-up ES (p = 0.000). However, initial injury severity, accompanying injury type, and main lesion location were not statistically associated with spontaneous recovery (p > 0.05).
Conclusions
Spontaneous recovery may be possible even in severe traumatic BPI. Multiple factors should be considered when predicting the clinical course of traumatic BPI.
Similar content being viewed by others


References
Barman A, Chatterjee A, Prakash H, Viswanathan A, Tharion G, Thomas R. Traumatic brachial plexus injury: electrodiagnostic findings from 111 patients in a tertiary care hospital in India. Injury. 2012;43:1943–8.
Dubuisson AS, Kline DG. Brachial plexus injury: a survey of 100 consecutive cases from a single service. Neurosurgery. 2002;51:673–82.
Rorabeck CH, Harris WR. Factors affecting the prognosis of brachial plexus injuries. Bone Jt J. 1981;63:404–7.
Midha R. Epidemiology of brachial plexus injuries in a multitrauma population. Neurosurgery. 1997;40:1182–9.
Chuang T-Y, Chiou-Tan FY, Vennix MJ. Brachial plexopathy in gunshot wounds and motor vehicle accidents: comparison of electrophysiologic findings. Arch Phys Med Rehabil. 1998;79:201–4.
Ferrante MA. Brachial plexopathies: classification, causes, and consequences. Muscle Nerve. 2004;30:547–68.
Giuffre JL, Kakar S, Bishop AT, Spinner RJ, Shin AY. Current concepts of the treatment of adult brachial plexus injuries. J Hand Surg. 2010;35:678–88.
Shin AY, Spinner RJ, Steinmann SP, Bishop AT. Adult traumatic brachial plexus injuries. J Am Acad Orthop Surg. 2005;13:382–96.
Dumitru D, Zwarts MJ. Brachial plexopathies and proximal mononeuropathies. In: Dumitru D, Zwarts MJ, editors. Electrodiagnostic medicine. Philadelphia: HANLEY & BELFUS, INC.; 2002. p. 790–8.
Tsai YA, Chuang TY, Yen YS, Huang MC, Lin PH, Cheng H. Electrophysiologic findings and muscle strength grading in brachioplexopathies. Microsurgery. 2002;22:11–5.
Tsai P-Y, Chuang T-Y, Cheng H, Wu H-M, Chang Y-C, Wang C-P. Concordance and discrepancy between electrodiagnosis and magnetic resonance imaging in cervical root avulsion injuries. J Neurotrauma. 2006;23:1274–81.
Dumitru D, Zwarts MJ. Electrodiagnostic medicine pitfalls. In: Dumitru D, Zwarts MJ, editors. Electrodiagnostic medicine. Philadelphia: Hanley & Belfus; 2002. p. 556–7.
Barman A, Chatterjee A, Prakash H, Viswanathan A, Tharion G, Thomas R. Traumatic brachial plexus injury: electrodiagnostic findings from 111 patients in a tertiary care hospital in India. Injury. 2012;43:1943–8.
Limthongthang R, Bachoura A, Songcharoen P, Osterman AL. Adult brachial plexus injury: evaluation and management. Orthop Clin N Am. 2013;44:591–603.
Garg R, Merrell GA, Hillstrom HJ, Wolfe SW. Comparison of nerve transfers and nerve grafting for traumatic upper plexus palsy: a systematic review and analysis. J Bone Jt Surg Am. 2011;93:819–29.
Yang LJ-S, Chang KW-C, Chung KC. A systematic review of nerve transfer and nerve repair for the treatment of adult upper brachial plexus injury. Neurosurgery. 2012;71:417–29.
Bengtson KA, Spinner RJ, Bishop AT, Kaufman KR, Coleman-Wood K, Kircher MF, et al. Measuring outcomes in adult brachial plexus reconstruction. Hand Clin. 2008;24:401–15.
Ahmed-Labib M, Golan JD, Jacques L. Functional outcome of brachial plexus reconstruction after trauma. Neurosurgery. 2007;61:1016–23.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Seong Hoon Lim, M.D., Ph.D., Jung Soo Lee, M.D., Ph.D., Yeo Hyung Kim, M.D., Tae Woo Kim M.D., and Kyoung Min Kwon, M.D. declare that they have no conflicts of interest.
Ethical approval
The study was reviewed and approved by the institutional review board of our institution (Ethical approval number: UC16RISI0083). For this type of study, formal consent is not required.
Funding
All authors did not receive any funding from institutions.
Rights and permissions
About this article

Cite this article
Lim, S.H., Lee, J.S., Kim, Y.H. et al. Spontaneous recovery of non-operated traumatic brachial plexus injury. Eur J Trauma Emerg Surg 44, 443–449 (2018). https://doi.org/10.1007/s00068-017-0810-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-017-0810-x