
Abstract
The term ‘state of the art” applied to medical technology should stimulate consideration of medical objectives as well as comparison of similar equipment. A communications model of the consult process is presented and examined using the diagnostic radiologists as the example. Examples of computer applications relating to the model are discussed, and some future possibilities for using computers to enhance the consultant's ability to meet medical objectives are suggested.
Similar content being viewed by others

References
Shannon, R. H., and Ball, M. J., A patient-oriented classification of medical data.Biosci. Commun. 2:282–292, 1976.
Kemeny, J. G.,Man and the Computer. Scribner, New York, 1972, p. 54.
Nilson, N. J., Artificial intelligence.Proceedings of the IFIP Congress 1974, North-Holland Publ., Amsterdam, 1974, pp. 802–805.
Shortliffe, E. H.,Computer-Based Medical Consultations, American Elsevier, New York, 1976, pp. 28–32.
Warner, H. R., Olmstead, C. M., and Rutherford, B. D., HELP—A program for medical decisionmaking.Comput. Biomed. Res. 5:65–74, 1972.
Rosati, R. A., McNeer, J. F., Starmer, C. G., Mittler, B. S., Morris, J. J., and Wallace, A. G., A new information system for medical practice.Arch. Intern. Med. 135:1017–1024, 1975.
Lodwick, G. S., The application of computers in diagnostic radiology.Curr. Probl. Radiol. 5:29–33, 1976.
Lang, G. S., State-of-the-art of computer-assisted radiology information/reporting systems.CRC Crit. Rev. Bioeng. pp. 221–250, June 1975.
Lusted, L., Evaluating the efficacy of radiological procedures.Models in Metrics for Decision Makers (K. Snappr, ed.), Information Resources Press, Washington, D.C., 1977.
McNeil, B. J., Keeler, E., and Adelstein, S. J., Primer on certain elements of medical decision making.N. Engl J. Med. 293:211–215, 1975.
McNeil, B. J., Varady, M. S., Burrows, B. A., and Adelstein, S. J., Measures of clinical efficacy.N. Engl. J. Med. 293:216–221, 1975.
Zwicky, G. and Gordon, S. C., Impact of a shared computer system in radiology department.Proceedings of the 4th Conference of Computer Applications in Radiology, American College of Radiology, Chicago, Ill. 1975, pp. 422–425.
Dietrich P. A., The computer-based medical record and the radiologist.The Problem-Oriented System (J. W. Hurst and H. K. Walker, eds.), Medcom, New York, 1972, p. 264.
Brooks, R. A., and DiChiro, G., Theory of image reconstruction in computed tomography.Radiology 117:561–572, 1975.
Lodwick, G. S., The application of computers in Diagnostic radiology.Curr. Probl. Radiol. 5:33–50, 1976.
Normandie, L. F., and Spiegel, P. K., A computerized exposure system.Radiology 120:575–581, 1976.
Brolin, I., Radiologic reporting.Acta Radiol. [Suppl.] 323, 1973.
Pendergrass, H. P., and Bauman, R. A., Computers in radiology at Massachusetts General Hospital.Radiol. Clin. North Am. 9:141–148, 1971.
Simon, M., and Leeming, B., Computerized radiology reporting using coded language.Radiology 113:343–349, 1974.
Wheeler, P. S., Simborg, D. W., and Gitlin, J. N., Johns Hopkins radiology reporting system.Radiology 119:315, 1976.
Lodwick, G. S., The application of computers in diagnostic radiology.Curr. Probl. Radiol. 5:14–53, 1976.
Mani, R. L., A computer-assisted radiographic reporting systems utilizing mark-sense format.Proceedings of the 3rd Conference on Computer Applications in Radiology, American College of Radiology, Chicago, 1972, pp. 58–67.
Kolodny, G. M.: A new system of radiology reporting.CRC Crit. Rev. Clin. Radiol. Nucl. Med. pp. 187–197, Dec. 1975.
Weintraub, H. D., Worcester, J., Resnic, M. S., and Kolodny, G. M., Clinical evaluation of the Rapid Telephone Access System for radiology reporting.Radiology 121:349–352, 1976.
Schultz, Jr., Cantril, S. V. and Morgan, K. G., An initial operational problem-oriented medical record system — For storage, manipulation, and retrieval of medical data.The Problem Oriented System. (J. W. Hurst and H. K. Walker, eds.), Medcom, New York, 1972, pp. 201–250.
Cantril, S., personal communication, 1976.
Author information
Authors and Affiliations
Additional information
Editorial comment
The basis model of a diagnostic process is greatly simplified by the single concept of “consulting” applied to radiologist and physician interaction. Much of radiology is performed as a function of protocol based on medical—legal boundaries and operates as a separate service to the patient with or without a physician's direct consent. To exemplify this open-ended structure, one should consider additional options: society's decision to examine, e.g., the Armed Forces entrance examination; institutional demands to examine, e.g., insurance physical examinations; legal decisions to examine, e.g., admission chest films; financial decision to examine, e.g., screening centers.
It would be most interesting to see a full-blown systems analysis of this process of consultation as modeled for radiology with all the various complexities graphically displayed in flowchart format. One must realize that the process described is dynamic and, therefore, has transfer rates and kinetic constants. Some of the processes are going strictly in one direction, whereas others have feedback and may actually go backward.
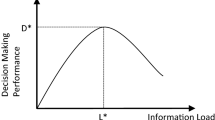
A second aspect of this dynamic service is output; one must be aware of a feedback loop to the consultant for retest and additional procedures. Here one is asking the questions: How much information flows back? How much does the radiologist tell the physician? Is the private physician able to make a competent decision for further testing? More questions can be asked about output: How many data get lost? How much is misinterpreted even though it is properly printed and graphically displayed? What are the kinetic constants of assimilation of these data into the individual decision-making process? Based on our experience, it would be very difficult to contrive a design that could evaluate a diagnostic radiology information package without having a complete picture of the process and all its possible outcomes. One would also need some idea of the volume and kinetic behavior of this model as a living and viable entity. Observed in this light, the criteria for success might be drastically changed to cover obvious deficiencies that would exist in the composite picture.
Dr. Shannon has given a general model, in his own words, one which can be applied to other specialties. We, in pathology, fill a role similar to that of diagnostic radiology, yet have even a wider front door for receiving requests and a broad spectrum of output. An adequate description of our consultative role has required extensive documentation to cover all the avenues of implied or delegated responsibility. In our particular case, only after we had documented our current system and all its intricacies were we able to deal intelligibly with a second-generation approach to improve process control and integration. We suggest that this same review would be necessary for those attempting to improve their radiology systems as one component of the complex entity called the medical data base.
Rights and permissions
About this article
Cite this article
Shannon, R.H., Grams, R.R. Computers and diagnostic radiology. J Med Syst 1, 37–49 (1977). https://doi.org/10.1007/BF02222875
Issue Date:
DOI: https://doi.org/10.1007/BF02222875